Islam et al., 1990*0 – 24 hours 176.7 ± 72.1101.7 ± 50.2 42.4 %
Islam et al., 1990* 24 – 48 hours 184.7 ± 108.390.8 ± 40.250.8 %
Molla, et al., 1985 0 – 24 hours 204c 155d24.0 %
Sabchareaon et al., 1989* 0 – 24 hours 2046.3 g stool/day 775.8 g stool/day 62.1 %
Greenough, 1987* 0 – 24 hours 325 105 67.6 %
Greenough, 1987* 24 – 48 hours 150 6556.7 %
The Complex
That Simply Works
Best
Concentrated High Energy Electrolyte Rehydration Solution
Rapidly Replenishes Fluids & Electrolytes
Promotes Extra Fluid Absorption To Help Reduce Volume & Duration of Diarrhea
Unique Complex Carbohydrate-Base
Reduces Osmotic Penalty
Helps Correct Metabolic Acidosis
Allows Continuous Feeding of Milk
Provides Multiple Sources of Energy
Ideal for Calves Suffering from Diarrhea
TECHNICAL TRAININGFor Use With
CALF SCOURS
21 Normandy Drive,
Lake St. Louis, MO 63367, USA
Tel: (636) 625-1884 Fax: (636) 625-1747
Advantages:
Complex Carbohydrate, No Osmotic Penalty:
Complex Carbohydrate (polymer linked glucose molecules) facilitates rapid absorption of electrolytes and water into the blood without "osmotic penalty" (e.g. water flowing undesirably from the blood, back to the gut), which can result with dextrose (simple sugar glucose)-based solutions.
Complex Carbohydrate allows concentrated glucose to be stored in the lumen, for transport, before crossing the gut wall, because chemical bonding reduces osmolarity of glucose. Extra glucose means extra absorption of fluid secreted in the bowel, to reduce volume and duration of diarrhea.
Complex Carbohydrate is instantly absorbed as glucose when its bonds are broken at the gut wall. Sodium and water are immediately absorbed with the glucose into the blood, without any time to experience osmotic pressure or penalty.
Complex Carbohydrate sustains energy and nutritional balance.
Increase water absorption for blood volume maintenance and balanced pH.
Provide metabolic energy for body functions.
Ideal For Periods Of Scours To Fight Dehydration
Uses two solutes (Complex Carbohydrate – maltodextrin, and glycine) which quickly transport electrolytes and water, even when the primary sodium-water channel is disrupted by disease.
Palatable/Digestible/Efficient
Strawberry/banana flavored for appetite appeal.
Contains no bicarbonate, won't interfere with milk digestion.
Balances pH, won't interfere with feed digestion.
Mixes easily in warm water (105-120o F). Will require slightly more mixing than dextrose solutions. But this little extra effort will go far in the long run.
Concentrated High Energy Electrolyte Rehydration Solution
U.S. – Mix 5 oz (70 g) of C.H.E.E.R.S.™ powder with warm water (110o F) to make two quarts of solution. Enclosed scoop (4 oz. Liquid) holds approximately 2.5 oz dry C.H.E.E.R.S. powder. Use two level scoops full of dry C.H.E.E.R.S. powder to make two quarts of solution.
Metric – Mix 148 grams (5.25 oz) of C.H.E.E.R.S.™ powder with warm water (43o C) to make two liters of solution. Enclosed scoop (4 oz. Liquid) holds approximately 70 grams dry C.H.E.E.R.S. powder. Use two heaping scoops full of dry C.H.E.E.R.S. powder to make two liters of solution.
Feeding Directions:
U.S. – For Calves Requiring Electrolytes and Fluid – Feed 2 quarts (4 lb) of electrolyte solution per calf 2-3 times daily, 2 to 3 hours after feeding.
Metric – For Calves Requiring Electrolytes and Fluid – Feed 2 liters (2 kg) of electrolyte solution per calf 2-3 times daily, 2 to 3 hours after feeding.
Continue Feeding Milk or Milk Replacer
C.H.E.E.R.S. does not interfere with milk digestion. Continue feeding milk replacer when using this product. Feed C.H.E.E.R.S.™ electrolyte solution through esophageal feeder, if needed. Research shows calves fed milk, even during periods of scours, gain more weight than calves fed electrolytes only.
Product Code: 9898 4B Net Weight: 25 lb (11.34 kg) heat-sealed, poly-lined paper bag
Product Code: 9898 34 Net Weight: 10 lb (4.54 kg) Plastic rectangular pail with E-Z open lid and carrying handle
Product Code: 9898 L7 Net Weight: 3.5 lb (1.59 kg) Plastic square pail with E-Z open lid
Product Code: 9898 ER Net Weight: 6 kg (13.23 lb) Plastic pail with lid
Overview of Scours
Defining Scours
In a normal gut, as needed, water flows to the lumen of the intestine for the purpose of aiding digestion and back to the blood for the purpose of absorbing nutrients, maintaining blood pH and distributing oxygen throughout the body.
Scours is a general term for a disease process which results from a disturbance in flow of water, back and forth, between the small intestine and the blood.
Scours may progress through four stages, if left unchecked (Dr. Vermeire’s “Four D’s of Scours“):
1) Diarrhea
2) Dehydration
3) Depression
4) Death from acidosis
Causes Of Scours
The causes of scours are varied and include exposure to viruses, bacteria, protozoa or various nutritional and digestive problems. These microbial or nutritional causes of scours can often interrupt and damage (usually temporary if corrected quickly) the internal system at the villi and crypt cell level that regulate continuous back and forth flow of water between the intestinal lumen and the body (via the blood).
The normal calf transports about 100 liters (about 26.4 gallons) of water across the gut wall into the intestine and reabsorbs this 100 liters back into the body via the blood, throughout the day.
Diarrhea
When water gets "stuck" in the lumen and cannot get back into the body, this excess water becomes part of the stool and appears as diarrhea. The loss of body fluids via stool leads to dehydration.
Recognizing Symptoms Of Scours
Dehydration 0-5% of body weight:
Not easily detectable
Dehydration 6-8% of body weight:
Loose, watery stool
Droopy ears
Slight recession of eyeballs
Dehydration 9-11% of body weight:
Eyes clearly sunken into sockets
Lack of skin elasticity of neck and eyelid determined by how fast skin snaps back when pinched
Depression (Symptom of metabolic acidosis - blood pH less than 7.2)
- Losing ability to suck and blink
- Lack of tactile response-skin twitching and head movement
- Lack of response to quick hand movements near eyes
Lack of ability to stand
Cold extremities due to reduced blood circulation.
Dehydration 12-15% of body weight:
Coma
Death
Understanding Digestion & Absorption
DIGESTION
Nutrients must be separated out from food and made water soluble before they can be absorbed. By digestion we mean first reducing food to its constituent parts, into a form suitable for absorption by the body fluids: the insoluble or barely soluble macromolecular organic nutrients such as proteins and complex carbohydrates are transformed into water soluble compounds of low molecular weight by enzymes in the digestive juices.
Enzymes are synthesized in glands in the mouth, stomach, intestine and pancreas. Each digestive enzyme is responsible for the chemical splitting of a particular type of nutrient.
ABSORPTION
Almost all the nutrients in food, including minerals and vitamins as well as the end products of digestion, are absorbed in the small intestine. When digestion is complete, the proteins, fats and complex carbohydrates are changed into amino acids, shorter chain fatty acids (up to C10) and monosaccharides which can pass through the mucous membrane villi cells along the "brush border" of the small intestine and into the blood vessels. This process is called absorption. Only when nutrients are absorbed are they considered to be nutritionally "in the body".
A Close Look At The Small Intestine: Site Of Absorption
VILLI, projections formed by folds in the lining of the small intestine, contain cells that absorb water and nutrients from the intestinal lumen, or cavity. These villus cells send the nutrients to the blood or lymph. Other projections (microvilli) on the cells (details at right) increase the absorptive area. At the base of the villi are crypt cells, which also participate in digestion.
The Sodium-Water Absorption Systems
Absorption of water occurs at the gut wall via sodium or solute-sodium systems of transport:
1. The Sodium Transport System
Water can be absorbed via a primary channel whereby water ions follow sodium and other electrolyte salts across the semi-permeable gut wall.
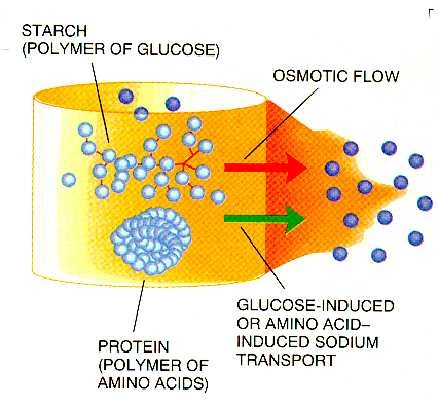
2. The Glucose or Amino Acid-Induced Sodium Transport System
An alternative, highly effective, auxiliary transport channel exists for sodium and water, when glucose is present. This auxiliary co-transport channels remain in operation even when the primary sodium-water channel is disabled from disease or stress.
The availability of this alternate channel for sodium and water was first recognized by modern science in the 1960's, in human studies. This discovery lead to the emergence of dehydration fighting, oral, dextrose (glucose) electrolyte products. However, because of osmotic pressure created by each glucose molecule, no more glucose than the proportionate amount of this solute found in normal blood can be included in the formulation...until now, with the introduction of C.H.E.E.R.S. and its special complex carbohydrate polymer bond advantage.
Crypt Cell Activity
At the base of the villi are specialized cells called "crypt" cells. The crypt cells work in cooperation with the villus cells during digestion to cycle fluid from the blood to the intestinal lumen and back again to the blood.
Crypt cells extrude chloride ions (Cl-) into the lumen (1) triggering a parallel flow of sodium (Na+) and then water and other ions from the blood into the lumen (2).
Villus Cell Activity
Later, villus cells pump sodium into the spaces between villus cells (3), thereby generating a compensatory movement of sodium into the cells from the lumen
(4, 5) and because, as a rule, water follows sodium, the direction of the water flow is reversed now towards
the blood (6)
Electrolytes such as sodium and chloride make use of the villus cells primary sodium-absorbing channel (a).
Additionally, sodium and water can be transported into
the body, in the presence of particular solutes, such as glucose, through an alternate transport system (b). Recent research has also shown that certain amino acids can further enhance transport of sodium and water via
co-transport channels in the presence of glucose, even when the primary sodium and water system is not able
to function, as during periods of scours, stress or nutritional upsets.
The Limitations Of Dextrose-Based Solutions
Osmosis, Osmotic Pressure & Osmotic Penalty
When two solutions are separated by a water-permeable membrane, such as the gut wall, the solution with a higher concentration will attract water from the less concentrated solution, in order to balance the amount of solutes on both sides of the membrane, to create equilibrium.
The higher concentration of solute on one side of a water-permeable membrane creates "osmotic pressure". The process by which water flows to balance the concentrations is called "osmosis". When water flows in an undesirable direction, this is called "osmotic penalty".
Limitations of Standard Dextrose Electrolyte Solutions:
Dextrose-based oral rehydration treatments (ORTs) must only contain up to as much glucose concentration as is found in normal blood or risk high osmotic pressure. When glucose is provided at the level of concentration of normal blood, the co-transport system for glucose and sodium is activated and induces an osmotic flow of water towards the dehydrated blood which drags along additional ions. Dextrose-based solutions can only exactly replace water, sodium and other ions lost from dehydrated blood. However, they cannot generate extra fluid absorption, to reduce the extent or duration of diarrhea.
Why Extra Glucose Cannot Be Added: Osmotic Penalty
Increasing the amount of glucose in standard dextrose-based electrolyte formulas might at first seem a reasonable way to speed fluid and electrolyte absorption. Yet, introducing extra glucose would, in fact, be dangerous.
An increase in concentration of glucose on the lumen side, greater than that of normal blood, would make the solution hypertonic and osmotic pressure or tendency to gain water on the lumen side would increase, in an effort
by the system to dilute the solute and create
equilibrium. The semi-permeable gut wall would
allow water to flow undesirably from the blood into
the intestine, exacerbating any dehydration.
Tangible evidence of this process is seen when a dehydrated, perspiring athlete, on a very hot day drinks several hypertonic, sugar-based beverages in rapid succession. Initially, the athlete becomes faint as the concentrated sucrose draws fluid into the gut lumen before it is subsequently reabsorbed, over time.
The Complex Carbohydrate Advantage
C.H.E.E.R.S.: Low Osmotic Pressure - Complex Carbohydrate Base
The Complex Carbohydrate used in C.H.E.E.R.S., is a polymer chain of linked glucose molecules. In solution, only the unbound ends of molecules contribute to osmotic pressure while the molecules within are neutralized by the chemical links. That explains why each molecule, whether it is one glucose unit or a chain of glucose units, adds the same amount of osmotic pressure. C.H.E.E.R.S. reduces osmotic pressure compared to dextrose solutions because the glucose units are bound together within our Complex Carbohydrate molecule. By formulating with a Complex Carbohydrate instead of simple sugar dextrose (glucose) we can deliver more glucose to the lumen for sustained sodium and water transport, without high osmotic pressure and risking osmotic penalty.
Why C.H.E.E.R.S. Works Better
The rates of hydrolysis (splitting of bonds) of Complex Carbohydrate bonds by pancreatic amylase and brush-border hydrolases are approximately equal to the rate at which the end product (glucose) is absorbed. Instant absorption of high levels of individual glucose molecules, which are released only at the intestinal wall, virtually eliminates time for the system to experience osmotic penalty. Therefore, it is now possible, without any increase in osmolarity of luminal contents, and allows us to deliver a relatively higher concentration of glucose, markedly broaden the activity of glucose-induced sodium transport channel and draw extra water and electrolytes into the blood than with dextrose-based solutions. This extra fluid absorption is drawn from the bowel, to reduce the volume of watery stool and possibly also the duration of diarrhea.
C.H.E.E.R.S.ControlComments
Dehydration Score
Day 1 1.61.0C.H.E.E.R.S. Calves started out slightly worse than control calves
Dehydration Score
Day 50.0 0.0No difference
Depression/Acidosis Score
Day 12.21.0 C.H.E.E.R.S. Calves started out slightly worse than control calves
Depression/Acidosis Score
Day 50.21.5 C.H.E.E.R.S. calves BETTER than control calves
Fecal Consistency Score
Day 12.82.6 No difference
Fecal Consistency Score
Day 51.82.5 C.H.E.E.R.S. calves BETTER than control calves
Number of calves5 5 Same number of calves
Day 1
Number of calves5 2 C.H.E.E.R.S. calves BETTER than
Day 5control calves
Death Loss 0 3/5 = 60% C.H.E.E.R.S. calves BETTER than control calves
What the scores mean:
Dehydration score = Skin tenting score (0-2 with 2 worse) + Eyeball recession score (0-2 with 2 worse)
Depression score = Suck reflex score (0-2 with 2 worse) + Menace reflex score (0-2 with 2 worse) +
Tactile response score (0-2 with 2 worse) + Ability to stand score (0-2 with 2 worse)
Fecal consistency score (1-4 with 4 worse)
For all scoring measures, the lower number is better than higher numbers.
Did You Know C.H.E.E.R.S. …
Contains Organic Salts to Correct Acidosis Without Interfering With Digestion
C.H.E.E.R.S. was developed utilizing the most recent research from around the world. C.H.E.E.R.S. effectively corrects metabolic acidosis by using organic salts (Sodium Acetate, Sodium Propionate, Calcium Acetate, Sodium Citrate) rather than using sodium bicarbonate. Unlike sodium bicarbonate, organic salts do not interfere with milk digestion. This superior system allows the continuous feeding of milk or milk replacer while using C.H.E.E.R.S. for rehydration of scoured calves.
Carbohydrate Technology is Based On Human Research Studies
Superior human electrolyte solutions have included carbohydrate formulas for almost 20 years, yet only unique C.H.E.E.R.S. Electrolyte Nutrient Product applies the osmotic benefits of Complex Carbohydrates to use with calves and other animals. Yes, Complex Carbohydrate costs a little more and, yes, it takes just a bit longer to mix but the performance results will be well worth the small additional investment.
Below are several key human studies demonstrating the highly effective results of using Complex Carbohydrates to reduce the volume of diarrhea compared to dextrose-based electrolyte solutions.
Stool volume Compairson: Dextrose vs. Complex Carbohydrte Electrolyte Solutions in Humans
a, b Treatments with unlike superscripts are different (P<.05)
c, d Treatments with unlike superscripts are different (P<.01)
* Significance levels not reported
Key Findings: In all cases, stool volume was lower when complex carbohydrate was used than when dextrose was used. Complex carbohydrate was superior to dextrose in every case.
C.H.E.E.R.S. References
Athanassious, Raafat, Gregoire Marsolais, Robert Assaf, Serge Dea, Jean-Paul Descoteaux, Suzanne Dulude, Claude Montpetit. 1994. Detection of bovine coronavirus and type A rotavirus in neonatal calf diarrhea and winter dysentery of cattle in Quebec: Evaluation of three diagnostic methods. Can Vet J 35:163-169
Bernardini, T.M.M., D.D. Kress, V.M. Thomas, and D.C. Anderson. 1996. The effect of scours on calf weaning weight. Proc. West Sec Am Soc Anim. Sci. Vol 47, Mont. Agric Exp Sta J. Series No. J-5029
Booth, Amanda J., DVM, MVSc, and Jonathan M. Naylor, BVSc, PhD. 1987. Correction of metabolic acidosis in diarrheal calves by oral administration of electrolyte solutions with or without bicarbonate. J. Am Vet. Med. Assoc. 191:62-68
Bywater, R.R., PhD, BVMS, MRCVS. 1977. Evaluation of an oral glucose-glycine-electrolyte formulation and amoxicillin for treatment of diarrhea in calves. Am J Vet Res 38:1983-1987
Bywater, R.J. 1979. Oral scour formulations with citrate. United States Patent 4,164,568. Aug. 14, 1979.
Bywater, R.J. PhD, MSc, BVMS, MRCVS. 1980. Comparison between milk deprivation and oral rehydration with a glucose-glycine-electrolyte formulation in diarrhoeic and transported calves. Vet. Record 107:549-551
Bywater, R.J. 1982. Pathophysiology and treatment of calf diarrhoea. XII World Congress of Diseases in Cattle, Amsterdam, Netherlands. p 291-297
Bywater, R.J., PhD, BVMS, MRCVS. 1983. Evaluation of an oral glucose-glycine-electrolyte formulation and amoxicillin for treatment of diarrhea in calves. Am J Vet Res 38:1983-1987
Bywater, R.J., G.H. Palmer and A. Stanton. 1982. The influence of milk replacer, water or an oral fluid replacer on the absorption of antibiotics on preruminant calves. XII World Congress of Diseases in Cattle, Amsterdam, Netherlands. p 301-304
Cleek, J.L., BS and R.W. Phillips, DVM, PhD. 1981. Evaluation of a commercial preparation for oral therapy of diarrhea in neonatal calves: administration by suckling versus intubation. J. Am Vet. Med. Assoc. 178:977-981
Davis, Dr. Carl L. Water and electrolyte balances in young animals as affected by diarrhea. Milk Specialties Co, Dundee, Illinois.
Demigne, C., C. Remesy, and F. Chartier. 1982. Interest of acetate in oral glucose-electrolytes formulations for treatment of dehydration in diarrhoeic calves. Proc. XII World Congress of Diseases in Cattle, Amsterdam, Netherlands. p 305-308
Demigne, C., C. Remesy, F. Chartier and D. Kaligis. 1983. Utilization of volatile fatty acids and improvement of fluid therapy for treatment of dehydration in diarrheic calves. Ann. Rech. Vet. 14:541-547
Demigne, C., C. Remesy, F. Chartier, and J. LeFaivre. 1981. Effect of acetate or chloride anions on intestinal absorption of water and solutes in the calf. Am J Vet Res 42:1356-1359.
Effertz, Nita. 1994. Go with the flow. Trash those scour pills, it's the fluids that stop the losses. Beef Today, March 94 p 25-28
Fettman, Martin J., DVM, PhD, Patricia A. Brooks, BS, Karen P. Burrows, BS, Robert W. Phillips, DVM, PhD. 1986. Evaluation of commercial oral replacement formulas in healthy neonatal calves. J. Am Vet. Med. Assoc. 188:397-401
Field, Michael, MD. 1977. New strategies for treating watery diarrhea. New England Journal of Medicine 297:1121-1122
Fisher, Edward W. 1971. Hydrogen ion and electrolyte disturbances in neonatal calf diarrhea. Ann NY Acad Sci. 176:223-230
Garthwaite, B.D., J.K. Drackley, G.C. McCoy, and E.H. Jaster. 1994. Whole milk and oral rehydration solution for calves with diarrhea of spontaneous origin. J. Dairy Sci. 77:835-843
Gorrill, A.D.L., and J.W.G. Nicholson. 1969. Effect of added bulk on growth, nutrient utilization, digestive system and diarrhea in calves fed milk replacer. Can J. Anim. Sci. 49:305-313
Greenough, William B. II, MD. 1983. Super ORT. J. Diar Dis Res. 1:74-75.
Greenough, William B. II, MD. 1987. Status of cereal-based oral rehydration therapy. J. Diarrhoeal Dis. Res. 5:275-278
Groothuis, D.G., and A.S.J.P.A.M. van Miert. 1987. Salmonellosis in veal calves. Some therapeutic aspects. The Vet. Quarterly 9:91-96
Groutides, C. and A.R. Michell. 1990. Evaluation of acid-base disturbances in calf diarrhoea. Vet. Record 126:29-31
Groutides, C.P. and A.R. Michell. 1990. Intravenous solutions for fluid therapy in calf diarrhoea. Res Vet. Sci. 49:292-297
Haider, R., A.K. Azad Khan, S.K. Roy, N. Dewan, A.N. Alam, and D. Mahalanabis. 1994. Management of acute diarrhoea in diabetic patients using oral rehydration solutions containing glucose, rice, or glycine. Brit Med J 308:624-626
Hammer, Heinz F., Kenneth D. Fine, Carol A. Santa Ana, Jack L. Porter, Lawrence R. Schiller, and John S. Fordtran. 1990. Carbohydrate malabsorption. Its measurement and its contribution to diarrhea. J. Clin. Invest. 86:1936-1944
Heath S.E., J.M. Naylor, B.L. Guedo, L. Petrie, C.G. Rousseaux and O.M. Radostits. 1989. The effects of feeding milk to diarrheic calves supplemented with oral electrolytes. Can. J. Vet. Res. 53:477-485
Kasari, Thomas R. DVM, MVSc. 1990. Metabolic acidosis in diarrheic calves: the importance of alkalizing agents in therapy. Veterinary Clinics of North America: Food Animal Practice 6:29-43
Lew, Judy F, MD, Roger I Glass, MD, PhD, Raymond E Gangarosa, MD, MPH, Ivan P Cohen, Caryn Bern, MD, and Christine L. Moe, PhD. 1991. Diarrheal deaths in the United States, 1979-1987. A special problem for the elderly. JAMA 265:3280-3284.
McLean, D.M., BRurSc, and L.F. Bailey, PhD. 1972. The effectiveness of three treatments for scouring in calves. Aust Vet J 48:336-338
Merck Veterinary Manual, sixth ed. 1986. Fluid and electrolyte imbalance. p 354-357
Michell, A.R. 1974. Body fluids and diarrhoea: dynamics of dysfunction. Vet Record 94:311-315
Michell, A.R. 1979. The pathophysiological basis of fluid therapy in small animals. Vet Record 104:542-548
Michell, A.R. 1989. Practice Tip. Oral and parenteral rehydration therapy. Vet Rec supplement In Practice. 11:96-99
Michell, A.R. 1991. Calf diarrhoea quiz. Vet. Record 128:576
Michell, A.R., H.W. Brooks, D.G. White, and A.J. Wagstaff. 1992. The comparative effectiveness of three commercial oral solutions in correcting fluid, electrolyte and acid-base disturbances caused by calf diarrhoea. Br. Vet J. 148:507-522
Molina, Susana, MD, Carolina Vettorazzi, MD, Janet M Peerson, MS, Noel W. Solomons, MD, and Kenneth H. Brown, MD. 1995. Clinical trial of glucose-oral rehydration solution (ORS), rice-dextrin-ORS, and rice-flour-ORS for the management of children with acute diarrhea and mild or moderate dehydration. Pediatrics 2:191-197
Naylor, Jonathan M. 1987. Severity and nature of acidosis in diarrheic calves over an under one week of age. Can Vet J. 28:168-173
Naylor, Jonathan M. 1989. A retrospective study of the relationship between clinical signs and severity of acidosis in diarrheic calves. Can Vet J. 30:577-580
Naylor, Jonathan M. 1990. Oral fluid therapy in neonatal ruminants and swine. Veterinary Clinics of North America: Food Animal Practice 6:51-67
Naylor, Jonathan M, and Taryn Liebel. 1995. Effect of psyllium on plasma concentration of glucose, breath hydrogen concentration, and fecal composition in calves with diarrhea treated orally with electrolyte solutions. Am J. Vet Res. 56:56-59
Pellerin, Charles, Jan Van Den Hurk, Jacqueline Lecomte, and Peter Tussen. 1994. Identification of a new group of bovine viral diarrhea virus strains associated with severe outbreaks and high mortalities. Virology 203:260-268
Perry, H.B., T.E. Johnson, B.L. Miller, M.A. Fowler, and R.M. DeGregorio. 1998. Effect of added copper sulfate in calf milk replacer on performance and scouring of calves. J. Anim. Sci. Vol. 76, Suppl. 2 P. 72
Phillips, Robert W. 1982. Normal intestinal function in the calf. Proc. XII World Congress of Diseases in Cattle, Amsterdam, Netherlands. p 267-273
Phillips, R.W., and K.L. Knox 1969. Water Kinetics in enteric disease of neonatal calves. J. Dairy Sci. 52:1664-1668
Phillips, Robert W., and Lon D. Lewis. 1972. Milk replacers: evaluation and use. Bov Pract. 7:28-33 and 7:79
Phillips, Robert W., Lon D,. Lewis, and Kirvin L. Knox. 1971. Alterations in body water turnover and distribution in neonatal calves with acute diarrhea. Ann NY Acad Sci. 176:231-243
Place, N.T., A.J. Heinrichs, and H.N. Erb. 1998. The effects of disease, management, and nutrition on average daily gain of dairy heifers from birth to four months. J. Dairy Sci. 81:1004-1009
Roenfeldt, Shirley. 1995. Scouring calves need milk, too. Dairy Herd Management. December 1995. p 22-24
Sperotto, G., F.R. Carrazza, and E. Marcondes. 1977. Treatment of diarrheal dehydration. Am J Clin Nutr 30:1447-1456
Tremblay, Robert R.M., DVM, DVSc. 1990. Intravenous fluid therapy in calves. Veterinary Clinics of North America: Food Animal Practice 6:77-101
Verschoor, Jaap, and Cary R. Christensen. 1990. Fluid therapy with specific mucopolysaccharides. Veterinary Clinics of North America: Food Animal Practice 6:69-75
Virtala, A.-M. K., G.D. Mechor, Y.T. Grohn, and H.N. Erb. 1996. The effect of calfhood diseases on growth of female dairy calves during the first 3 monthes of life in New York state. J Dairy Sci. 79:1040-1049
Wanner, M., G. Ziv, J. Nicolet, U.P. Noelpp, and H. Roesler. 1981. Experiments with the double isotope single-injection method for determining glomerular filtration rate and effective renal plasma flow in veal calves. Research in Vet Sci. 30:239-240